Clinical and Equity Implications of
Braidwood v. Becerra
AFFORDABLE CARE ACT PREVENTIVE SERVICES PROVISION
Preventive services can help people avoid acute illness, identify and treat chronic conditions, prevent cancer or lead to earlier detection, and improve health (1). These services enable individuals to maximize their health, and often mitigate the need for more serious and expensive medical interventions in the future (2). The preventive services provision of the Affordable Care Act (ACA) requires non-grandfathered private health insurance plans to provide coverage for certain preventive services without co-payments, coinsurance, or deductibles (1). This policy was intended to enhance healthcare access, reduce disparities in the use of preventive services and improve health outcomes for millions of Americans.
The preventive services provision requires nearly all private health plans to provide first-dollar coverage for specific preventive services, including:
- Items and services receiving an “A” or “B” rating from the U.S. Preventive Services Task Force (USPSTF)
- Immunizations recommended by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC)
- Recommendations for preventive care and screenings issued by the Women’s Preventive Services Initiative and the Bright Futures for Children Program (3) supported by the Health Resources and Services Administration (HRSA)
These federal administrative agencies issue evidence-based recommendations for clinical services for which there is high certainty of moderate to substantial health benefits. For example, there are 46 USPSTF “A” or “B” rated recommendations for high-value screenings, immunizations, and preventive medications. To reflect ever-evolving preventive care needs, the Task Force frequently reviews new evidence, resulting in either a new recommendation, updates to existing recommendations, or a call for more research (4). As new recommendations are issued or updated, coverage must commence in the next plan year that begins on or after exactly one year from the recommendation’s issue date (5).
Incentivizing use of preventive care services by providing first-dollar coverage has the potential in certain circumstances to reduce aggregate spending. From a payer perspective, investments in prevention in the early and middle decades of life, when people are more likely to be covered by private health plans, may lead to Medicare beneficiaries entering the program at age 65 in better health – potentially leading to lower overall Medicare costs (1).
IMPACT OF THE ACA PREVENTIVE SERVICES PROVISION
The U.S. Department of Health and Human Services estimated in 2022 that 152 million Americans had access to additional preventive care with zero cost-sharing through private health insurance, along with an estimated 61 million Medicare beneficiaries, and 20 million adult Medicaid expansion enrollees (2). Closer analysis of 2018 claims data estimates that six in 10 adults (approximately 100 million) and seven in 10 children with private insurance used at least one preventive service covered by the ACA in a typical year, prior to the COVID-19 pandemic (6). A May 2023 KFF analysis reported that about one in 20 privately insured people – about 10 million people in total – received at least one ACA preventive service or drug in 2019. Prescription of statins, which are used to treat people at risk of cardiovascular disease, was the most utilized preventive service.
As one of the most popular features of the ACA, nearly 1 in 4 Americans believe that preventive care is one of the most important health benefits for commercial insurance plans to cover (7). In addition, 62% of Americans believe that it is “very important” that the preventive service coverage requirement to stay in place (8).
IMPACT OF REMOVAL OF COST-SHARING: REVIEW OF LITERATURE
Prior to the ACA, financial barriers deterred use of clinical care and resulted in large racial differences in the use of clinical preventive services among People of Color (POC) adults relative to White adults (9). Since the ACA preventive services provision took effect, research has shown that providing preventive services without cost-sharing has improved vaccination rates, increased screening rates for certain chronic conditions and cancers, and improved access to preventive and life-saving medications – especially among individuals for whom affordability was a key barrier pre-ACA (10).
For example, the rate of mammography screening for breast cancer among Hispanic women and the rate of colonoscopy screening for colon cancer among both Hispanic and Black adults increased faster over time, when compared with White adults after the implementation of the ACA (9).
More recent research suggests that increases in preventive services utilization disproportionally benefit specific underserved populations, including low-income individuals, Medicare beneficiaries lacking supplemental insurance, and those with high levels of cost-sharing for a service (11). While the majority of peer-reviewed studies showed increases in the use of fully covered preventive services, studies that included socioeconomic status reported more substantial increases in utilization of preventive services in financially vulnerable patients as compared to those with higher income (Table 1).
A robust evidence base reveals that minority populations and low-SES individuals stand to benefit the most from cost-sharing elimination, as reduction of financial barriers leads to increased access to care and reduced health disparities (11).
TABLE 1: Peer-reviewed studies examining the impact of eliminating consumer cost-sharing that included socioeconomic status
| REFERENCE | HEALTH PLAN | UTILIZATION OUTCOME |
|---|---|---|
|
CHOUDHRY ET AL. (2014) |
Private, employer-sponsored health plan |
Cost-share removal increased medication adherence and reduced rates of major vascular events or revascularization for vulnerable non-White populations. The impact was greater for non-White populations compared to White populations. |
|
COOPER ET AL. (2017) |
Medicare (fee-for-service) |
After implementation of the ACA, breast cancer screening rates increased, and the gap in receipt of mammography between the lowest and highest SES strata narrowed. |
|
DALTON ET AL. (2018) |
Private, employer-sponsored health plan |
Post-ACA, rates of long-acting reversible contraception (LARC) insertion increased, but changes in utilization depended on baseline costs prior to ACA. Those who had the largest decline in out-of-pocket costs had the largest increase in uptake of LARC. |
|
FEDEWA ET AL. (2015) |
Medicare |
Rates of colorectal cancer screening and colonoscopy increased, with the largest increase limited to respondents with lower SES, lower levels of education, and Medicare – the population subgroup that is expected to benefit the most from the ACA. |
|
RICHMAN ET AL. (2015) |
Medicare |
Post-ACA, use of colonoscopy for colorectal cancer screening increased among those who lived in poverty and those with only original Medicare coverage (no private insurance/Medigap, Medicaid, or MA), showing that cost-share elimination benefits specific populations more. |
|
TOSEEF ET AL. (2020) |
Medicare |
Nationwide, among beneficiaries with traditional Medicare only, who stood to gain the most from eliminating cost-sharing for preventive services, the percentage of women receiving clinical breast exams rose post-ACA. |
BRAIDWOOD V. BECERRA
Despite its positive impact and the progress made toward equitable access to preventive health care over the past decade, the ACA continues to be one of the most contested laws in U.S. history (12). Most recent litigation, Braidwood Management v. Becerra, was brought forth by plaintiffs in Texas who assert that (1) the requirements in the law for specific expert committees and a federal government agency to recommend covered preventive services is unconstitutional, and that (2) the requirement to cover preexposure prophylaxis (PrEP), medication for HIV prevention, violates their religious rights via the Religious Freedom Restoration Act (RFRA) (3).
In September 2022, Texas U.S. District Court Judge Reed O’Connor ruled that the preventive service requirement for USPSTF recommendations was unconstitutional because the task force members are neither appointed by the President nor confirmed by the Senate, thereby violating the Appointments Clause (13).
The Court found that the ACIP for vaccines and the HRSA for Women’s Preventive Services delegations are not in violation of the Appointments Clause since the Secretary of HHS effectively has the authority to ratify or not the ACIP and HRSA recommendations (3).
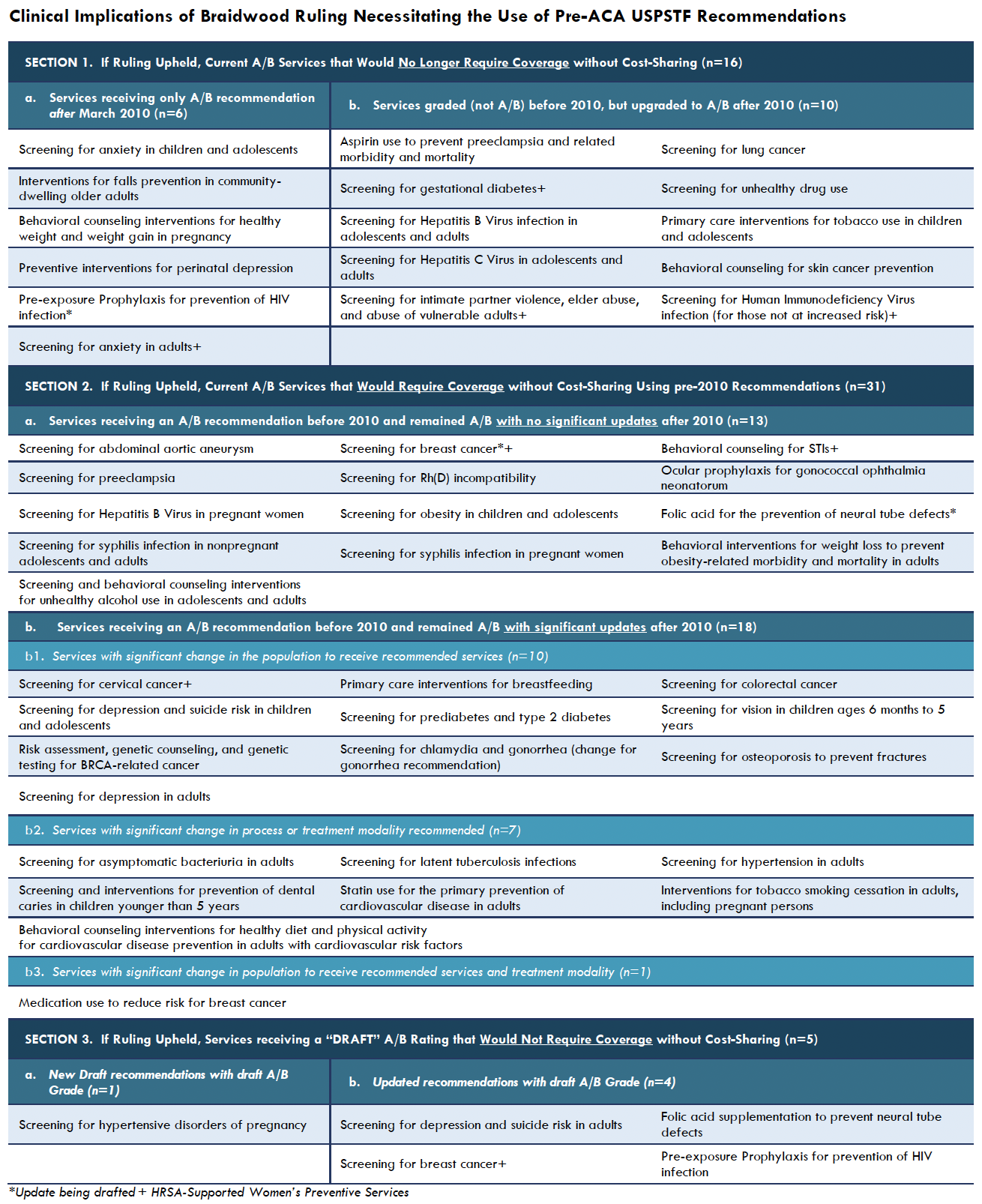
In the subsequent March ruling, Judge O’Connor ruled that the mandate to fully cover services receiving a USPSTF “A” or “B” grade on/after the signing of the ACA on March 23, 2010, is unconstitutional. This ruling immediately overturned full coverage of recommended services added since March 2010, including screening for anxiety, screening for depression and suicide risk, pre-exposure prophylaxis (PrEP), perinatal and gestational screenings and interventions, as well as several other recommendations with significant health benefits. This ruling also requires plans to continue to provide access to services that received an “A” or “B” USPSTF grade before March 23, 2010, without cost-sharing (Table 2) (14).
The federal government appealed this decision, and on May 15, 2023, the 5th Circuit Court of Appeals issued an administrative stay of the district court’s ruling, allowing the federal government to continue enforcing the preventive services requirement while the 5th Circuit considers the Department of Justice’s motion for a stay pending appeal (3).
While the current litigation is focused on private insurance, a decision eliminating the requirement of first-dollar coverage for preventive services could also impact people in Medicaid expansion plans and Medicare beneficiaries, dependent on the coverage decisions of individual states and future administrations (2). While this lawsuit challenging the preventive services provision plays out in court, most U.S. health insurers plan to continue offering free preventive health services, according to a letter sent to Democratic lawmakers from leading insurers and industry organizations, including America’s Health Insurance Plans, the Blue Cross Blue Shield Association and the American Benefits Council.
IMPLICATIONS OF THE BRAIDWOOD RULING
If the courts uphold the Braidwood ruling that no-cost coverage be provided only for USPSTF “A” or “B” recommendations made prior to March 2010, a dramatic change in coverage of impacted preventive services may result, potentially leading to coverage decisions based on evidence inconsistent with the most up-to-date scientific research (14).
New/Updated USPSTF A/B Recommendations
Of the 46 USPSTF services that are currently fully covered, one-third received an A/B rating after 2010, potentially disqualifying them from coverage without cost-sharing (e.g., Pre-exposure Prophylaxis (PrEP) for prevention of HIV infection, screening for anxiety in children and adolescents, and screening for lung cancer – see Table 2, Section 1) (14). Additionally, 6 new and updated services currently receiving a “draft” A/B rating would no longer require coverage without cost-sharing (e.g., screening for anxiety in adults, screening for depression and suicide risk in adults, and screening of hypertensive disorders of pregnancy – see Table 2, Section 3). Furthermore, all future USPSTF A/B new and updated recommendations may not be covered without cost-sharing.
USPSTF Recommendations Pre-ACA
While required no-cost coverage of USPSTF A/B recommendations made prior to March 2010 has been perceived as a victory by public health advocates, the reality is much more complex. If Braidwood is enforced, the older, pre-ACA recommendations would be covered without cost-sharing, but the updated recommendations would not require full coverage (see Table 2, Section 2). For example, in 2008, an “A” recommendation for colorectal cancer screening suggested screening average risk adults aged 50-75 years. In 2021, this recommendation was updated to lower the age of screening for average risk adults to 45, thereby extending no-cost screening to an additional 20 million Americans each year (14).
Example of Draft USPSTF Recommendations
Most recently, the USPSTF has issued a draft updating the recommendation for breast cancer screening. The most recent recommendation, released in 2016, suggests that all women aged 50-74 years receive breast cancer screenings every other year. The May 2023 draft recommendation suggests that biennial screening mammography should start for women at average risk for breast cancer beginning at age 40. This recommendation is based on new and more inclusive science about breast cancer in people younger than 50, as the rate of breast cancer among women ages 40-49 increased 2% per year, on average, from 2015-2019 (15). The task force estimates that the new recommendations could prevent at least one additional breast cancer death for every 1,000 women (16).
TABLE 2: Clinical Implications of Braidwood Ruling Necessitating the Use of Pre-ACA USPSTF Recommendations
Note: Scroll to see full table or click link above for PDF
Judge O’Connor’s decision is unpopular among both the public and patient advocacy groups. In a recent Morning Consult survey, half of U.S. adults – a majority of Democrats and a plurality of Republicans – reported that they do not approve of the Braidwood ruling, and patient advocacy groups continue to stress the implications of creating uncertainty over the coverage of potentially life-saving care for hundreds of millions of people (17).
Evidence shows that requiring people to pay out-of-pocket for preventive services – even if the cost is relatively low – can stop them from seeking routine care altogether, possibly leading to more complex and costly health conditions that might have been more treatable or less costly if diagnosed earlier (6,7). According to a recent consumer survey, 37% of adults said they “definitely” or “probably” expect to delay or avoid heath care due to potential costs following the ruling, and at least 2 in 5 adults said that they are not willing to pay for preventive services that are currently fully covered by the ACA (7,17).
INITIAL EMPLOYER/INSURER RESPONSES TO THE BRAIDWOOD RULING
If overturned through federal courts, the clinical, economic, and equity benefits of expanded access to preventive care currently afforded by the ACA preventive services provision will be markedly diminished once insurers are again able to require cost-sharing for these critical services (2,18). Though it is unclear how plans would respond to the removal of this requirement, once there is no longer a legal obligation to cover preventive care, employers will have the option to reduce coverage, impose cost-sharing, or change policies regarding preventive care coverage over time (10).
In an October 2022 Employee Benefit Research Institute (EBRI) survey including 25 employers representing 1.2 million covered lives, 20% of employers reported that they might impost cost-sharing on previously covered services if permitted, with 8% responding that they “would,” and 12% responding “it depends.” (19). More recently, a National Alliance survey polling 30 employers representing 1.5 million workers indicates that about 72% of employers expect to continue providing coverage for preventive services at 100%. Six percent of employers expect to be more selective, and 22% don’t know how they will approach coverage for preventive care services (Figure 1).
FIGURE 1: Employer Surveys Assessing Likelihood of Imposing Cost-Sharing on Preventive Services
Financial Implications
While the impact of reintroducing cost-sharing for preventive services has the potential to be financially burdensome and worsen disparities, recent claims data analysis finds that the correlated savings for plans would result in minimal impact to overall plan spending. Findings demonstrate that the costs of covering select preventive services are very low. If, for example, employers were to introduce 20% member cost-sharing for breast, cervical, and colorectal cancer screenings – some of the most widely sed “A”- and “B”- rated preventive services – they would reduce their spending by .27%. Similarly, if employers were to impose 20% cost-sharing on previously fully covered preventive medications, it would reduce their spending by only .3% (Table 3) (13).
TABLE 3: Cost of Select Preventive “A” and “B” Rated Services, 2019
| PREVENTIVE SERVICE | TOTAL COST PER USER | % OF MEMBERS UTILIZING SERVICE | % OF TOTAL COST | EMPLOYER SAVINGS FROM 20% CO-INSURANCE |
|---|---|---|---|---|
|
Breast Cancer Screening |
$332 |
10% |
0.5% |
0.11% |
|
Cervical Cancer Screening |
$39 |
9% |
0.10% |
0.01% |
|
Colorectal Cancer Screening* |
$990 |
4% |
0.70% |
0.15% |
|
HIV PrEP Medication |
$13,814 |
0.20% |
0.40% |
0.08% |
|
Statins (Ages 40-64) |
$151 |
8% |
0.20% |
0.04% |
|
Breast Cancer Preventive Drugs (Ages 35-64) |
$237 |
1% |
0.02% |
0.00% |
|
Contraceptives |
$470 |
9% |
0.70% |
0.14% |
|
TOTAL |
|
|
2.62% |
.53% |
* Not including facility fees, pathology, or anesthesia
HIV=Human Immunodeficiency Virus; PrEP=Pre-Exposure Prophylaxis
Source: The Impact of Covering Select Preventive Services on Employer Health Care Spending. EBRI Fast Facts. 2022.
CONCLUSION
Given the robust evidence on the detrimental clinical and equity effects of cost-sharing on care utilization, imposing cost-sharing for preventive care is likely to reverse the progress made by Section 2713 and the intensifying efforts to reduce socioeconomic, racial, and LGBTQ+ health disparities; a concern that should be weighed carefully by policymakers (13). The burden of losing first-dollar coverage for preventive services will fall disproportionately on lower-income individuals, historically marginalized communities, and those with multiple chronic conditions; many of whom are most likely to benefit from, but least able to afford, these necessary services (20,14).
REFERENCES
- ASPE Issue Brief. Access to Preventive Services without Cost-Sharing: Evidence from the Affordable Care Act. ASPE. 2022.
- Horstman C, Baumgartner JC, Shah Arnav. Millions Could Lose Access to Free Preventive Care Services. Commonwealth Fund. 2023.
- Sobel L, Ranji U, Pestaina K, Dawson L, Cubanski J. Explaining Litigation Challenging the ACA’s Preventive Services Requirements: Braidwood Management Inc. v. Becerra. 2023.
- https://www.uspreventiveservicestaskforce.org/uspstf/
- https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/uspstf-value-primary-care-fact-sheet-2021.pdf
- Amin K, Lissenden B, Carley A, Pope G, Claxton G, Rae M, Rakshit S, Cox C. Preventive Services Use Among People with Private Insurance Coverage. KFF. 2023.
- Zipp R. Many Americans Are Likely to Skip Preventive Care if ACA Coverage Falls Through. Morning Consult. 2023.
- Kirzinger A, Montero A, Hamel L, Brodie M. 5 Charts About Public Opinion on the Affordable Care Act. KFF. 2022.
- Thorpe KE. Racial Trends in Clinical Preventive Services Use, Chronic Disease Prevalence, and Lack of Insurance Before and After the Affordable Care Act. AJMC. 2022;28(4):e126-e131.
- Skopec L, Banthin J. Free Preventive Services Improve Access to Care. Urban Institute. 2022.
- Norris HC, Richardson HM, Benoit MAC, Shrosbree B, Smith JE, Fendrick AM. Utilization Impact of Cost-Sharing Elimination for Preventive Care Services: A Rapid Review.
- Murphy N, Hughes S. Fact Sheet: Braidwood v. Becerra Case on Preventive Services. Center for American Progress. 2023.
- The Impact of Covering Select Preventive Services on Employer Health Care Spending. EBRI Fast Facts. 2022.
- Chopra Z, Fendrick AM. Clinical Implications of the Braidwood Ruling: Use of Pre-ACA Task Force Recommendations. Health Affairs Forefront. 2023.
- SEER* Stat Databases: November 2021 Submission. National Institutes of Health; National Cancer Institute – Surveillance, Epidemiology, and End Results Program. 2021.
- Bendix A. Screen all women for breast cancer at 40, instead of 50, new guidelines say. NBC News. 2023.
- Zipp R. A Federal Judge’s Ruling to Block ACA Requirement for No-Cost Preventive Care is Unpopular. Morning Consult. 2023.
- Stone W, Summers J, Fendrick AM. Millions may lose free preventive health care after ruling by federal judge in Texas. NPR News; All Things Considered. 2023.
- EBRI Fast Facts. Will Employers Introduce Cost Sharing for Preventive Services? Findings From EBRI’s First Employer Pulse Survey. EBRI. 2022.
- Minemyer P. Judge blocks feds from enforcing ACA’s preventive care coverage mandates. Fierce Healthcare. 2023.