V-BID in Action: A Profile of Connecticut’s Health Enhancement Program
Value-Based Insurance Design (V-BID)—hailed as a “game changer” by the National Coalition on Health Care— refers to insurance designs that vary consumer cost-sharing to distinguish between high-value and low-value health care services and providers. V-BID entails (1) reducing financial barriers that deter use of evidence-based services and high-performing providers, and (2) imposing disincentives to discourage use of low-value care. Through the incorporation of greater clinical nuance in benefit design, payers, purchasers, taxpayers, and consumers can attain more health for every dollar spent. The University of Michigan Center for V-BID leads in research, development, and advocacy for innovative health benefit plans and payment reform initiatives.
Connecticut Seeks to Improve Health and Contain Costs
The State of Connecticut faced a projected budget gap of $3.8 billion in fiscal year 2012, and state employees were asked to help address the shortfall. The Governor’s Office and a coalition of unions representing state employees met throughout 2011 to discuss a wide range of topics, including the health plan covering active and retired state employees. The parties focused health care discussions on possibilities for improving health as a means to control long-term costs. Discussions involving unions, the Governor’s representatives, and the Connecticut Office of the State Comptroller led to the October 2011 launch of an uncommonly innovative initiative—the Health Enhancement Program (HEP).
Given the new and central role of beneficiary accountability in this novel plan design, preliminary versions were carefully scrutinized and modified. Shortly after union ratification, open enrollment took place in October 2011. As designed and implemented, HEP incorporates clinically-nuanced elements of V-BID, eliminating barriers to specified evidence-based clinical services based on beneficiary demographics and medical history. This brief highlights some of HEP’s key features, as well as early results and lessons learned.
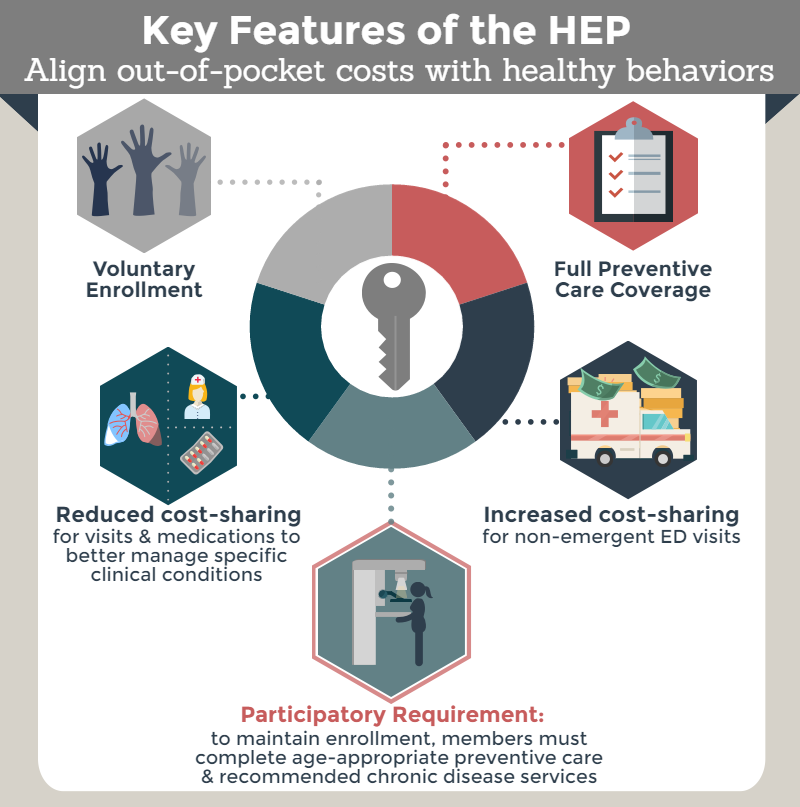
The Key Features of HEP
Prior to 2012, Connecticut’s state employee health plan did not distinguish between high-value services and low-value services in determining cost-sharing for beneficiaries. HEP is different.
Accountability. HEP rewards state employees, select retirees, and dependents who commit to a number of responsibilities. The “ask” of beneficiaries is as follows:
- Obtain specified age and gender-appropriate health risk assessments, evidence-based screenings, and physical and vision examinations;
- Undergo two dental cleanings per year;a and
- Participate in condition-appropriate chronic disease management services.b
Specified guideline-based clinical services are required of HEP enrollees with diabetes, high cholesterol, high blood pressure, heart disease, asthma, and chronic obstructive pulmonary disorder (COPD). There are provisions to exempt enrollees with unusual or special circumstances from requirements as appropriate.
Beneficiaries may be disenrolled from HEP if they do not adhere to the requirements outlined above. HEP strives to avoid this outcome through regular reminders and other forms of consumer outreach. Compliance with requirements is verified through claims data when possible, and written personal attestation when claims-based verification is not possible.
Incentives for Participants. HEP enrollees pay lower premiums and lower out-of-pocket costs at the point of service than beneficiaries who do not elect to participate. Specifically, HEP offers enrollees:
- Exemption from a health insurance premium surcharge imposed on non-enrollees (savings of $100 per month);
- No deductibles (potential annual savings of $350 per person, up to $1,400 per family);
- Reduction or elimination of copayments for medication associated with the management of chronic medical conditions (savings of up to $25 per prescription fill);c
- Elimination of copayments for office visits for chronic conditions (savings of $15 per visit); and
- Incentive payments of $100 annually if a member with a targeted chronic condition, including his/her dependents, complies with all of the HEP requirements in a given year.
To encourage prudent resource use, the new health plan imposes a $35 copayment for emergency department visits when there is a “reasonable medical alternative” and the beneficiary is not admitted to the hospital. This new provision applies to HEP members and non-members alike.
Results
Participants Respond to Incentives and Accept Accountability. About 98% of the approximately 54,000 eligible Connecticut state employees and retirees voluntarily enrolled in HEP. These individuals have overwhelmingly complied with program requirements: 98 percent of enrollees were deemed compliant at the end of each of the first two program years.iii
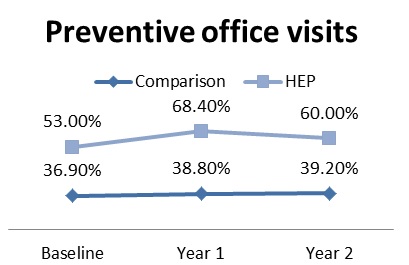
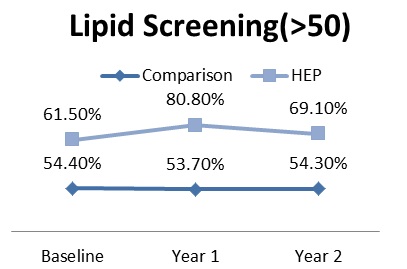
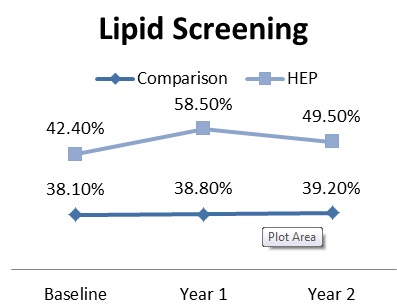
Clinically-Nuanced Incentives Increase Evidenced-Based Care and May Promote Favorable Changes in Utilization. According to the Connecticut State Comptroller, monthly primary care visits have increased from about 12,000 in July 2011 (prior to HEP launch) to about 21,000 in May 2012 (following HEP launch). Specialty care visits have decreased from about 24,000 in July 2011 to about 19,000 in May 2012. Monthly emergency room visits have fallen from about 3,500 in July 2011 to about 2,700 in May 2012. Adherence to heart disease, blood pressure, cholesterol, and diabetes medication has modestly improved since HEP’s launch.i High-value medical services, including preventive office visits and nearly all of the targeted preventive screenings, showed significant increases in both the first and second program years, relative to the comparison group.ii Preventive office visits increased by 13.5 percentage points in year 1 and 4.8 percentage points in year 2. Among preventive screenings, lipid screening for the population ages over fifty increased by 20.1 percentage points in year 1 and by 7.8 percentage points in year 2. Moreover, across all chronic conditions, there were considerable increases in physician office visits relative to the comparison group. The likelihood of having an office visit increased by 1.6 percentage points in year 1 and by 1.2 percentage points in year 2.iii
Increases in Health Care Spending May Be Slowing. Medical trend for HEP enrollees decreased from +13% in fiscal year 2011 to +3.8% in fiscal year 2012. The pharmacy trend remained flat, despite increased use of drugs to manage chronic disease.i Enrollees’ out-of-pocket spending dropped by about $66 in year 1 and about $76 in year 2.iii
[/fusion_builder_column]
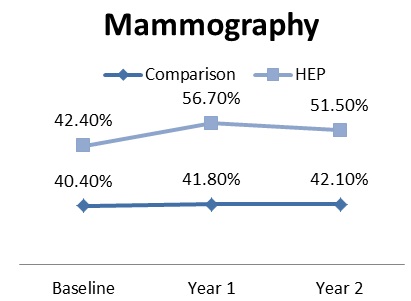
Changes in Utilization of Preventive Services Relative to Comparison Group: Baseline, Year 1, and Year 2
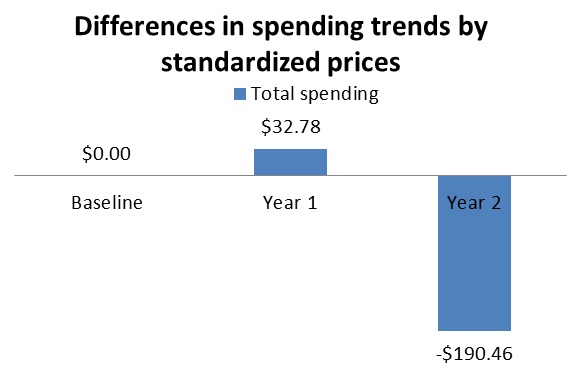
After removing the effects of different prices over time, despite a slight increase in spending in year 1 compared to baseline, there was a significant decrease of $190.46 in year 2 compared to baseline. The result suggests that positive difference maybe a result of growth of prices in Connecticut and not a result of changes in service utilization.
Lessons Learned
Stakeholders Can Collaboratively Design and Implement Innovative “Win-Win” Plans, Even Under Difficult Circumstances. The Connecticut experience demonstrates the ability of management and labor to reach consensus on significant changes to “business as usual” in health plan design, even in challenging fiscal environments. The success in launching HEP confirms that management and labor leaders can successfully engage third party administrators, pharmacy benefit managers, and other key stakeholders. Together, vested parties can overcome concerns about perceived intrusiveness, technical challenges, and other potential obstacles.ii
Consumers Will Commit to Health-Promoting Activities When Appropriately Incented. HEP has been broadly accepted, with nearly all eligible employees selecting the option.
Incentives Can Change Behavior. In accordance with a substantial body of literature, the new clinically-nuanced incentives appear to have affected use patterns among HEP enrollees. Early (albeit uncontrolled) data demonstrates favorable shifts, with promising implications for long-term health and health care spending. The Health Enhancement Program boosted the use of preventive services significantly across nearly all outcomes. For instance, lipid testing increased by 15.4 percentage points and mammography increased by 8.1 percentage points after one year of program implementation.
Despite apparent differences in results between the first two years of the program compared to baseline, occasional dips between year 2 and year 1 were identified. Screenings such as colonoscopies or Pap tests which occur less than once a year may reflect a natural decline in use.iii
Innovative Plan Designs are Imperfect, and Flexibility is Critical.
Given the rapid timeframe for roll-out, HEP leaders encountered implementation challenges, including clinician availability and establishment of vendor-administered programs. Leaders rapidly addressed these issues.
Next Steps, Implications, and Concluding Thoughts
Next Steps for Connecticut. Buoyed by early successes, the Connecticut stakeholders are seeking to evolve and expand HEP. Next steps include increasing use of patient-centered medical homes, improving awareness of emergency department alternatives, integrating with providers’ electronic health records, and extending HEP to municipal-level employees and dependents under age 26. Unions representing CT State employees approved new features to the HEP program for 2018. In addition to the existing V-BID elements of lowering or eliminating cost sharing for recommended preventive care and recommended clinical services for 5 common chronic diseases, it added:
- Preferred Networks: Zero copay for preferred PCPs and Specialists based on quality and cost
- Smart Shopper: Members will receive gift cards for having a list of procedures conducted at facilities that pass quality and cost measurements
- Site of Service: For imaging and labs, zero copay applies to preferred locations, 20% co-insurance for non-preferred in-network locations, and 40% co-insurance for out-of-network facilities
Broader Implications. When available, results from the V-BID Center’s evaluation of HEP will shed light on the clinical and financial impact of comprehensive, thoughtfully-designed V-BID programs. However, other employers and payers may consider adopting the Connecticut move from “volume to value” in whole or part even before definitive results are available. The concept of V-BID is expanding continuously, as public payers focus on services that have high clinical value. Connecticut is one of the seven states that are selected to participate in the Medicare Advantage Value-Based Insurance Design Model. This allows Medicare Advantage plans to offer supplemental benefits or reduced cost sharing to enrollees with certain chronic conditions specified by the Centers for Medicare and Medicaid Services (CMS). In light of the promising early findings and the broader evidence for V-BID, there is every reason to suspect that HEP-like approaches will produce dividends in terms of health, satisfaction, productivity, and affordability.
For other states. Findings from HEP have meaningful implications for other states. Due to their size, states as employers can affect benefits structures of enough consumers to prompt changes in health care markets. As the transition from a volume-driven to a value-based health care delivery system is continuing, the inclusion of clinically nuanced payment reform and consumer initiatives can improve quality of care and enhance the consumer experience.iii
References
a This applies only to those enrolled in dental coverage.
b The state’s two third party administrators offer disease management services for these conditions.
c Copayments for diabetes drugs are waived. Copayments for cholesterol, blood pressure, heart disease, asthma, and chronic obstructive pulmonary disorder medications are tiered at $0/$5/$12.50 (generic/preferred brand/other brand) versus $5/$10/$25 for non-HEP enrollees.
i Kevin Lembo. “Connecticut’s Health Enhancement Program.” Presentation to the National Academy for State Health Policy 25th Annual Conference (Baltimore, MD). 2012 October 15.
ii Chernew ME, Rosen AB, Fendrick AM. Value-Based Insurance Design. Health Affairs. 2007 March 1;26(2):w195–w203. http://content.healthaffairs.org/content/26/2/w195.full
iii http://content.healthaffairs.org/content/35/4/637.full.pdf