Originally Produced: November 2013 Updated: July 2019
Protecting Preventive Care Coverage in the Post-ACA Era
Preventive Care Coverage in the ACA:
Section 2713 of the Public Health Service Act as amended by the Patient Protection and Affordable Care Act (ACA) requires that issuers offering group or individual health insurance plans must provide coverage for specified preventive services without a beneficiary copayment or a contribution toward a deductible. This elimination of consumer cost-sharing applies only when these services are delivered by a network provider.
Determining Covered Preventive Services:
Congress selected three organizations to determine covered preventive services with the intent to include all segments of the population. These organizations are the United States Preventive Services Task Force, the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices, and the Health Resources and Services Administration. The current list of preventive services includes a variety of counseling services, immunizations, and screenings for cancer and treatable chronic diseases, such as diabetes and hypertension.
United States Preventive Services Task Force (USPSTF) is an independent body that does not necessitate approval from any Agency or Department before issuing a recommendation. The main responsibility of the USPSTF is to make recommendations on the use of primary preventive services through five level grades.
All services that receive an “A” or “B” rating from the USPSTF are defined as covered preventive services.
Advisory Committee on Immunization Practices (ACIP) is a group of medical and public health experts that develops recommendations on how to use vaccines to control diseases in the United States.
Immunization recommendations of the committee that have been adopted by the Director of the Centers for Disease Control and Prevention must be covered by applicable health plans.
Health Resources and Services Administration (HRSA) works to strengthen the health care workforce, build healthy communities, and improve health equity. The HRSA also works to provide health care to uninsured people, people living with HIV/AIDS, pregnant women, mothers, and children. The HRSA-supported women coverage guidelines, developed by the Institute of Medicine (IOM), ensure that women receive a comprehensive set of preventive services and fills gaps in other existing guidelines.
Women’s preventive health care – such as mammograms, screenings for cervical cancer, prenatal care, and other services – generally must be covered by health plans with no cost-sharing. However, the law recognizes the need to take into account the unique health needs of women throughout their lifespan.
Cost of care is explicitly not permitted in the selection of covered services. If a service is added to the covered services list, issuers have one calendar year from the date of the recommendation to include the new service without consumer cost-sharing. Services that are removed from the list are no longer required to be covered without cost-sharing by the issuer. However, to stay in compliance with other provisions in the ACA, the health plan is required to notify an enrollee 60 days before a co-payment, co-insurance, or deductible can be applied.[4]
Impact on Use of Preventive Services:
As of June 2019, 21 covered services have been identified for adults, 28 services for women (including pregnancy), and 31 services for children. Most of the recommendations are clinically nuanced, in that a specific population is clearly defined to receive each recommended service. Since the passage of the Affordable Care Act in 2010, the list of covered preventive services has been expanded to reflect current public health needs.
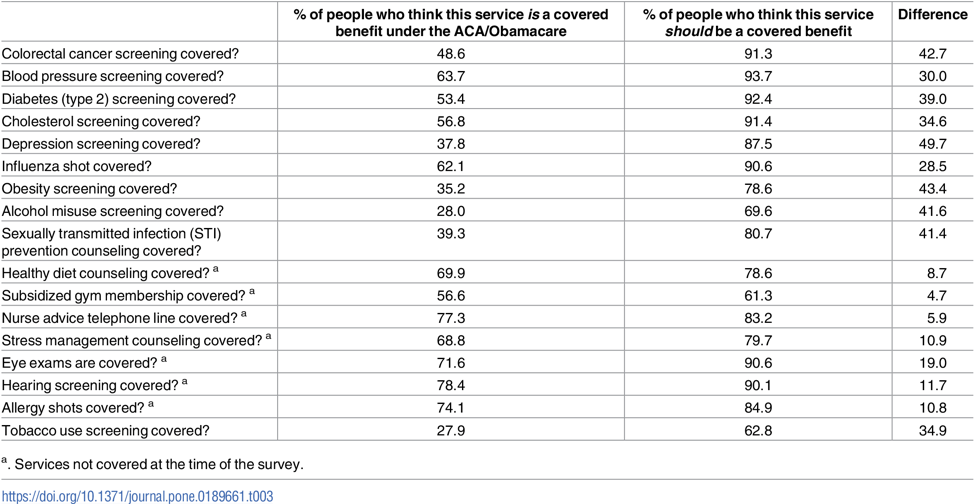
As of 2015, approximately 137 million Americans (108.8 million adults and 28.5 million children) received coverage for at least one free preventive service, such as a mammogram or flu shot.[5] Furthermore, utilization of preventive services is expected to increase as awareness of coverage grows. Currently, a significant number of Americans do not realize their preventive services are considered covered benefits under the ACA. [6] This may result in delay of care, poorer health outcomes, and more expensive health care.